Our PI Lisa is speaking on ‘Enduring Time – On Violence and Care’ as part of Alt_Cph_2020 on Wednesday, 16 September 2020 at from 5 – 6.30pm (UK time). This event is a Zoom webinar and is free to attend.
Lisa’s talk will be part of the Patterns of Resistance programme of events and you can sign up for the webinar here or visit the Alt-Cph_2020 site here.
In its early stages, the ongoing global pandemic laid bare the hidden structures of care and dependency that we often close our eyes to. COVID-19 also alerted us to our collective vulnerability and dependency – and the violence that so often goes hand in hand with care.
In her 2017 book ‘Enduring Time’ psychoanalyst and cultural theorist Lisa Baraitser diagnoses our present as a moment of suspended time. Between a traumatic past and a foreclosed future, we find ourselves in stuck time, a time closely connected to the time of care. In this talk Lisa Baraitser will be in dialogue with the curator Miriam Wistreich to use our current moment as a thinking space to consider the relationships between vulnerability, violence, resistance and care.
It is something of a foundational belief in the Sociology of Scientific Knowledge (and related fields) that knowledges are always shaped by the context within which they are constructed. Scientific knowledges are thus never independent of the social relations, economic structures, political pressures, ideological and tacit practices from which they emerged, and they are themselves cultural artefacts.[1]
Historians work with similar understandings about historical knowledge. Though articles or monographs do not routinely include historicisations of their own origins (though, note feminist histories like that by Catherine Hall and Carolyn Steedman), historians will usually recognise the circumstances of their text’s production in their acknowledgements.[2] Here they raise to the level of consciousness funding sources, intellectual interlocutors, social relationships and even some biographical detail to help make sense of where a particular work has developed.
The first page of acknowledgements by a certain author, who we shall call “M. Moore” to preserve their anonymity. That might be too obvious, let’s call them “Martin M.”
This is not to say that historians work unreflexively in relation to their origins, nor that they never publicly look to contextualise their own knowledge. Rather, they have tended to reflect most heavily on the relationship between past and present in historiographical and methodological texts.[3]
Recently the Waiting Times team has been thinking about how the current pandemic has been reshaping relationships to time (and care), which we will be sharing in a forthcoming dossier on COVID-19. It was in this context that I was reminded about E. H. Carr’s famous suggestion that history was an ‘unending dialogue between the present and the past’.[4] As historical and social subjects, in other words, historians are just as much a product of their particular time and place as those they write about, and our interpretations of the past will be inescapably influenced by our biographical, social and cultural relations.
Broadly speaking, historians have tended consider the relationship between the present of scholarship and the history produced in terms of large-scale social, economic and political formations and trends. How has a historian’s position in the social field shaped their view of the past? How might experiences of particular events or existence within specific cultural and political milieu shape the questions that are asked within research?
Regardless of how long the current measures of containment, delay and mitigation last, the impact of COVID-19 on psychosocial, economic and political life will likely be profound, and thus so will its effects on historical scholarship. Although it might be folly to think about precisely what these effects will be whilst we are still in the midst of the crisis – of a moment that might be an historical rupture and beginning of a new normal, or prove to be something far less monumental – it is nonetheless possible to consider how historical scholarship is already being reshaped. To explore how COVID-19 is already making history.
*
Perhaps the most overt ways in which the pandemic is influencing scholarship is in terms of disruption to intellectual networks and project temporalities.
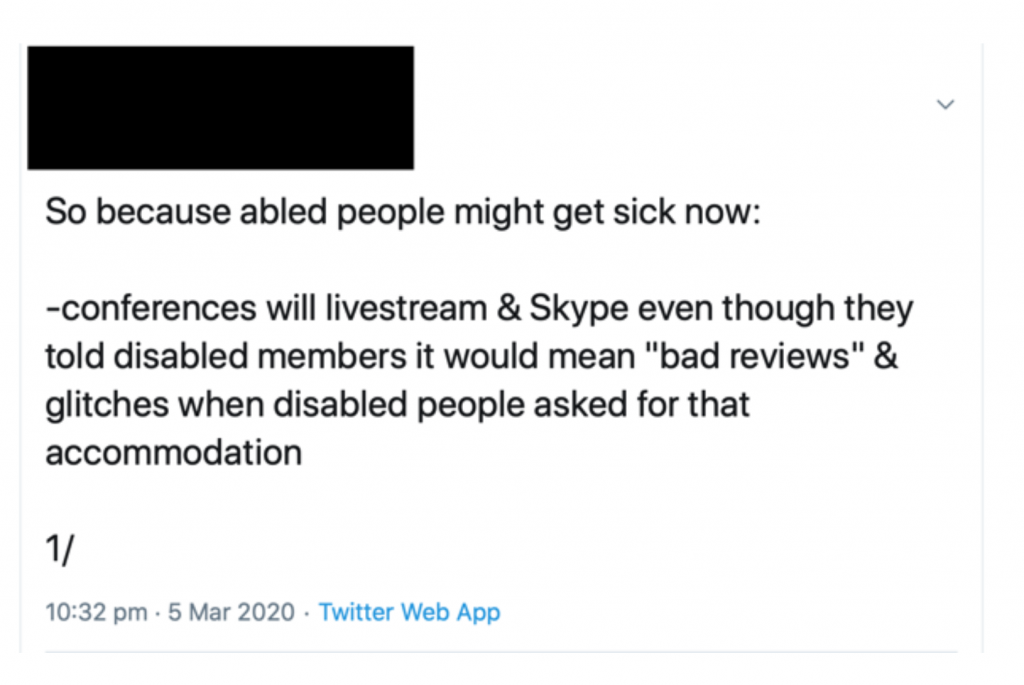
It might be tempting to point to the cancellation of conferences and reworking of seminars as a major consequence of COVID-19, and to consider how difficult it is to recreate opportunities for conversations and collaborations that tend to emerge from interaction outside of the formal conference room.
However, as disability activists and scholars with caring and familial responsibilities have pointed out, these issues are long-standing. It should be a matter of shame that it has taken a global pandemic to force able-bodied academics to think seriously about alternative ways of working, when this has been so long denied to colleagues unable to be physically present at large, and often distant, events.
Instead, a problem more directly caused by the pandemic is how COVID-19 has radically disrupted postgraduate and PhD research, and will potentially reduce the time available to undertake ongoing projects. At the time of writing, some funding bodies have so far shown a willingness to ensure no cost extensions in proportion to the disruption experienced, but considerable anxiety and uncertainty still exists, and the internal research leave and fixed contract arrangements of individual universities are being addressed idiosyncratically. The absence of a sector-wide response – of guaranteed secure employment at (or above) present levels of pay for casualised staff – has begun to generate political action under the banner of a Corona Contract. However, even if agreed, the personal circumstances of researchers change over time, and their capacity to undertake the same work may well be altered in the future. The knowledge produced will thus likely be substantively different as a result.
Similar analyses can be applied at the level of teaching. As was made clear at the Modern British Studies conference last August, history modules are already being shaped by the short fixed-term, zero-hour contracts spreading throughout academia. This has often reduced preparation time and opportunities for scholars to create their own offerings, leading to modules being inherited and reworked where possible by temporary staff. Individual universities have used COVID-19 as legitimation for laying off staff or refusing to continue contracts of fixed-term employees, and together with social distancing the landscape of teaching looks very different as a result.
*
Of course, the pandemic is also shaping the knowledge it is possible to produce at the level of sources and methods.
Closures of archives and libraries has ensured a majority of resources remain inaccessible, and de facto quarantine is altering the way we can undertake oral historical work. (Given that the direction of an encounter is often shaped by the embodied interaction of interviewer and interviewee constructing the interview together in the same room, it is likely that even online interviewing will produce different testimonies.)
Some textual and visual materials are available online, partly due to digitisation and partly due to the increasing use of the internet as historical object and source.
For instance, texts that are available digitally and made keyword searchable can grow in epistemological importance. Equally, engagement with uncatalogued materials becomes impossible, and the assessment of a source’s materiality – its physical substance, potential sensory responses, clues to its production – are also precluded or made more difficult. In this sense the pandemic risks compounding historians’ existing reliance on the narrow range of sources that have managed to survive, and which have often been produced by social elites and from positions of (often violent) power. We will require further innovation in approaches and methodologies to avoid reproducing historical violence in the present.
At the same time, public and political discourses of healthcare, disease and contagion – as well as experiences of illness and practices of social distancing and self-isolation – are also altering how we might read and interpret our sources.
At a very basic level, I am currently revisiting my own work on waiting rooms. Under present conditions, materials relating to concern of infection are beginning to stand out more. References to feeling disturbed or diminished by waiting with patients with ‘hacking coughs’, for example, take on greater resonance, as do recollections of the way such anxieties shaped practices of attending surgery and sharing the time of waiting.
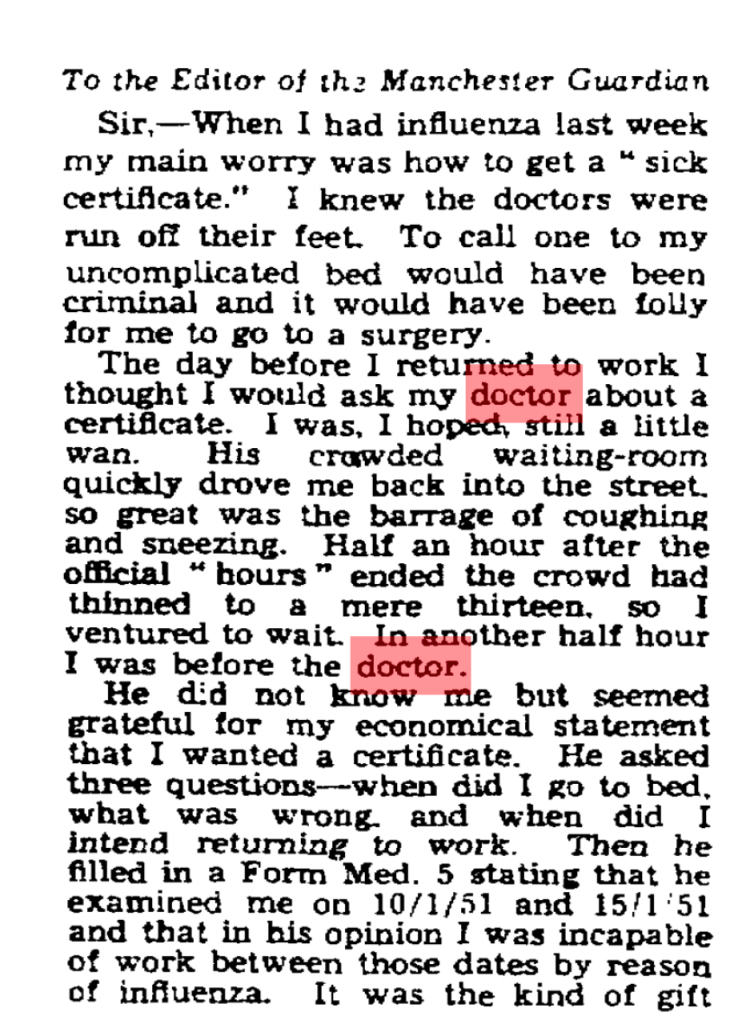
Take, for instance, one letter to the Manchester Guardian in 1951 about trying to collect a sickness certificate:
‘Ministries and medicine’, Manchester Guardian, 17 January 1951, p. 4
The day before I returned to work I thought I would ask my doctor about a certificate. I was, I hoped, still a little wan. His crowded waiting-room quickly drove me back into the street, so great was the barrage of coughing and sneezing. Half an hour after the official “hours” ended the crowd had thinned to a mere thirteen, so I ventured to wait. In another half an hour I was before the doctor.
Previously, I may have read this in terms of anxieties of waiting for – and consulting – the doctor when appearing healthy, in relation to the performativity of sickness. Equally, the source raises questions about the length of acceptable waiting, the responsibilities that doctors had to attend their patients after surgery hours, and the role of the medical profession in sick note certification. Even though I would have registered the disquiet with the waiting room as a source of infection, the fear of contagion would not have hit home in the same way.
Similar alterations in my interpretation have manifested in relation to GP’s frustrations with patients bringing in “dirt” to their waiting rooms. I have previously read such complaints in highly symbolic terms, in line with my interest in how discourses of dirt and cleanliness have been historically racialised and classed. Now, however, I am paying greater attention to dirt’s materiality. Though GPs’ irritations cannot be conceptually divorced from “dirt’s” cultural values, my own anxieties around the ongoing pandemic has made me appreciate the medical concern with hygiene embedded in GP’s choices of easy-to-clean materials for redecorating waiting in a period of regular infectious disease outbreaks.
Finally, even should the present proscriptions around “staying home” be eased, and libraries and archives swiftly reopen, the emotional experience of being in and using such spaces will also have been altered.
I already feel much more “exposed” simply going to a small supermarket, so I can only imagine that the experience of using public transport, sharing the space and time of research with others, and interacting with well-handled resources will be radically different for some time. To presume that such affective responses will not alter how I interact with historical sources (the time I can bear to be with them, how much more I rely on digitised versions) or the sorts of questions I will ask of them would be disingenuous.
Of course, even as I write many people literally cannot afford to avoid public transport or working away from home
*
There are, of course, much more complicated ways to think historically about epidemics, time and care in relation to scholars’ experiences of the present moment, and undoubtedly our teaching on history of disease and medicine modules will also be shaped by our students’ personal perspectives on their lockdown and social distancing.
Moreover, that I – and scholars like me – are only beginning to consider such questions seriously can itself be historicised.
This very reflection is the product of my having grown up in a period and place in which my privilege as a heterosexual, white (once working-, now solidly middle class) male living in Britain has afforded me protection – not simply from the epidemics that have tended to exist geographically and socially “elsewhere” (from HIV/AIDs to Ebola) but also from the structural violence that has consistently distributed disease disproportionately among the poorest and those most discriminated against in Britain (and globally). Even now, my positionality is proving protective, as underlined by reports that BAME communities are suffering disproportionate mortality from COVID-19.
Given the racial, class and gender disparities among the historical profession, I suspect that my experiences may be widely shared.
Nonetheless, whether explicitly discussed in acknowledgements, expressed within the subjects, questions and contours of research, reflected in how we organise and practice intellectual network formation, or manifest in the conditions within which teaching is delivered, the effects of COVID-19 on the present and future of historical scholarship will likely be widespread and significant. As such, though academic departments are by no means the only source of historical knowledge and narrative, it is fair to say that the present pandemic is also rewriting the past.
Notes
[1] For classics in the field and useful reviews: S. Shapin and S. Schaffer, Leviathan and the Air Pump: Hobbes, Boyle and the Experimental Life, (Princeton: Princeton University Press, 1985); S. Woolgar and B. Latour, Laboratory Life: The Construction of Scientific Facts, (Princeton: Princeton University Press, 1986); K. Knorr Cetina, Epistemic Cultures: How the Sciences Make Knowledge, (Cambridge, Mass: Harvard University Press, 1999); L. Daston and P. Galison, Objectivity, (New York: Zone Books, 2010).
[2] The most self-conscious example I have seen is the preface to a history on international development and the social sciences, which begins: ‘this book as much as the institutions which are its subject, comes out of a particular history, a certain intellectual climate, and specific funding possibilities’: R. M. Packard and F. Cooper (eds), International Development and the Social Sciences: Essays on the History and Politics of Knowledge, (Berkeley: University of California Press, 1997), p. vii. For examples of texts firmly grounded in the historian’s own positionality: C. Hall, White, Male and Middle Class: Explorations in Feminism and History, Cambridge: Polity Press, 2007 [1992]); C. Steedman, Landscape for a Good Woman: A Story of Two Lives, (London: Virago, 1986).
[3] For instance: A. Green and K. Troup, The Houses of History: A Critical Reader in History and Theory, Second Edition (Manchester: Manchester University Press, 2016); L. Jordanova, History in Practice, Third Edition, (London: Bloomsbury Academic, 2019).
[4] E. H. Carr, What is History?, Second Edition (London: Penguin, 1990 [1961]), p. 30.
As part of our ongoing partnership with Hospiscare, Messages in Bottles, we held three showcases of work produced by service-users of the Honiton day hospice.
These three events presented written stories, pictures, songs and short films made in our storytelling and story sharing collaborative workshops. We had participants – service-users, staff and researchers – as well as family, friends, carers and other members of the Hospiscare team come along for an afternoon of reading, thinking, talking and sharing at the King’s House day hospice in Honiton.
We also had plenty of tea, cake, laughter and the occasional tear.
Our next planned event is a tour of local libraries. We’ll be taking interactive displays of the stories to Honiton, Seaton, Sidmouth, Axminster and Exeter. We had planned to start this tour in April 2020, but we had to postpone for obvious reasons. Hopefully, libraries will re-open after the summer and we will be able to take take our show on the road then.
Until then, you can listen to some of the stories here.
In collaboration with Dr Arthur Rose (Bristol), Michael organised a series of lunchtime seminars for Occupational Therapy and Physiotherapy practitioners at the Royal Devon and Exeter hospital.
The workshops grew out of discussions with an OT nurse who attended a Waiting Times workshop at the Wellcome Centre for Cultures and Environments of Health. In addition to fostering links and dialogue between the research team and healthcare professionals, the seminars aim to provide humanities research-based ideas and inspiration for developing clinical practice, using the Waiting Times research as a major source of insight.
In November 2019, Michael shared stories, video and audio from the Messages in Bottles project he and Kelechi have worked on in partnership with Hospiscare.
In February 2020, Michael ran a workshop on how semiotic techniques can be applied to understand and improve upon communication, information exchange and partnership between patients and healthcare professionals in the clinical encounter.
Dr Rose, Michael and the OT team at RD&E will be planning future lunchtime seminars for the year 2020/21.
The Texture of Air: A History of Two Hospitals in Sound and Image
Image by Ben Evans James The Art Deco stairwell connecting the floors of the Eastman hospital
Stephanie Davis writes:
A few weeks ago, I attended the opening exhibition of ‘The Texture of Air’, a heritage project in honour of two old hospitals famous for their pioneering work introducing narrative therapy for children, snoring therapies and cochlear implants on the NHS amongst other things: the (old) Eastman Dental Hospital founded in 1931 and the (older) Royal National Ear, Nose and Throat Hospital (RNENT) opened in 1875. I learned that the project was commissioned three years ago after it was announced that the Eastman and the Royal National Hospitals would be moving from their ‘historic homes’ on Grey’s Inn Road to a new purpose built facility just around the corner. Today, this is the fully functioning New Eastman Hospital on Huntley Street whose foyer, with its 21st century hospital colour scheme and giant geometrical light fittings, I had the opportunity to visit since it served as the venue for the official opening of the exhibition.
I arrived expecting an oral history but the exhibition was much more than this. In addition to an archive of recorded conversations with hospital staff and patients captured over three years, there were films, photographs and artworks all inspired by the atmosphere and architecture of the buildings, the achievements of their inhabitants and the remnants of their working lives together. Accompanying it all was an orchestral score for a wind trio that had been composed especially. The composer, Nicole Robson spoke at the opening about how she had wanted to write a piece of music with the power to enchant its listeners in a way that would be reminiscent of the old (now deceased) Eastman hospital, with its maze of corridors, spiral staircases and the resounding footsteps of people coming and going from all directions.
Specialising as they did in the treatment of oral and aural conditions for many years, the two hospitals offer endless amounts of material for a project of this kind, leading to the discovery of resemblances between the work of trying to reconstruct the past creatively and the that of restoring lost hearing and speech by medical means. Affinities are drawn out in some of the more experimental field recordings featuring medical instruments or other specialist technology put to work in attempts to mediate the sounds of the hospital’s past. In one recording, the sound of an old television set is transmitted using induction coil pick-ups. In another, a much loved fountain on the hospital grounds is made audible from underwater using something called a hydrophone. Most recordings though, are of everyday noises made very simply by volunteers: fittings, machines, ways of life. They evoke the many worlds that disappeared along with the hospitals, of ancient doors swinging shut, an ornate lift grinding to a halt and patients chatting in the waiting room.
Several of the audio recordings have a strange echo-like quality of seeming to be simultaneously caught up in the present and the far flung past. The sounds of machinery whirring away in a non-existent lab for instance, the elongated beeps of the standard hearing test, the passing remarks of women stood together during a fire alarm test, are soundscapes that might belong to different decades or even to different centuries of the same institution. Whereas in the audio-visual archive, the old things of different eras are thrown together in the exhibition in a disorientating way with some of the images from the exhibition appearing almost ahistorical. Film footage of uniformed staff gazing into the camera and blanched out photographs of empty showroom clinics are cut off from anything that might bind them to a particular time period. They seem already to be disappearing into their own atmospheres as though detached from any actual past or future. The lidar scans showing cross sections of the hospital in fossil form also fall into this category of seeming to come from outside time altogether.
Another temporal grouping is reserved for things that have grown old during our own lifetime with a speed that seems to have been accelerated by the much older physical environment of their surroundings. An example of this is the image, shot in a side room of one of the old hospitals, of a heap of medical technology that can’t be older than twenty years being left to gather dust. The actual age of the materials and their connection to the present feels irrelevant. Like all the other things that fall into this category of discarded things from the long past of the institution, the objects lose any foothold in the recent past and get jumbled up with the things of other eras.
The circumstances surrounding the work might help to explain some of its anachronisms. Materials for the oral history were presumably being gathered in the final months and years just before the buildings were closed (demolished in the case of most of the Eastman Dental Hospital), and the work of collecting the past appears to have shared roughly the same timeline as the work of dismantling the two hospitals. There is at least one mention of this in recorded conversations when two women are overheard speculating hopefully about whether or not they will still get to see eachother after the crossover, “…we will still have time together, won’t we?”. But for the most part, nothing is said on the subject of the future. Its conspicuous absence lends the whole project an eerie quality, cutting it adrift from the present and making it seem as though the voices of staff and patients populating the institutions and now the archive, were never to leave the hospitals after those last days. Had somebody stayed around long enough to have overheard them making their way through the end of one era and into the start of another, the exhibition might have felt a little less haunted than it turned out to be, but the Texture of Air seems always to have been a project more interested in opening a portal to the past than in finding continuity with the future.
The project was led by Oral Historian, Laura Mitchison in association with Screen Deep and On the Record and featured the work of artists and the contributions of volunteers. A complete list of credits and the archive itself are available at https://www.thetextureofair.uk/
The exhibition will remain open for the public to view in the new Eastman hospital.
‘My own doctor is a charming man when one can eventually win an appointment to see him’: accessing the GP and the time of care in British general practice
Although, according to recent NHS data, on average only 1% of total primary care appointments were for home visits, the motion provoked a considerable backlash among patient groups, senior healthcare professionals, the press and Government ministers.
Critics broadly focused on the capacity for severely ill and immobile patients to access the GP, whereas supporters argued that GPs ‘no longer have the capacity to offer’ visits. At its heart, in other words, were questions about for whom and for what GPs should reasonably make time.
As my recent work on appointments systems is revealing, GPs’ time and patients’ rights of access to care have formed a central object in public debate since the foundation of the NHS. By contrast to the current proposals, however, the emergence of full-time appointments systems for surgery sessions in general practice generated far less initial resistance, despite affecting a far greater proportion of the practice population.
‘Much of the overwork of which doctors complain is due to lack of proper business methods’
The first decades of the NHS witnessed a considerable change in how people waited for a GP consultation.
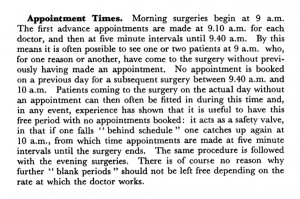
In the early 1950s, only 2% of British general practices employed full time appointments systems for their surgery sessions.[1] In the vast majority of practices, those patients wishing to see the doctor could simply arrive at the premises during surgery hours and wait to be seen in turn. Even practices with appointments systems quietly reserved part of the surgery session for patients arriving without an appointment.
From A. E. De La T. Mallett, ‘An appointment system in a group practice’, College of General Practitioners Research Newsletter, 3:8 (1955), 113-18
Finally, for those too ill to come to the surgery, visits were common; around a quarter of consultations on average occurred in patients’ homes.[2]
By the early 1970s this situation had dramatically altered. Around 80% of practices now employed full-time appointments systems.[3] Crucially, changes to NHS rules empowered doctors to defer treating patients who they felt were not in need of immediate attention. Patients were thus increasingly unable to access the doctor on demand without an appointment. A wait for the doctor might stretch to several days if one was unavailable immediately.
As with contemporary discussion around home visits, GPs’ concern with time pressure generated interest in appointments systems. Following the creation of the NHS, many GPs bemoaned having ‘much more work’ and feeling like they were ‘chasing [their] practice downhill all the time with no hope at present of ever catching up’.[4] As a result, many doctors sought organisational innovation to achieve ‘more economic use of … time and energy’.[5]
Notably, one particular attraction of new systems was that they might ‘reduce the demand for visits’, as reduced crowding and waiting times could make surgery attendance less taxing.[6] The time saved by reduced travelling could be put to use elsewhere.
Efficiency was not the sole factor motivating GPs to take up appointments systems, however. Traditional arrangements, for instance, could lead to late-running surgeries – any patient who arrived before doors closed had a right to be seen. As one satirical novel put it: ‘the patients came steadily to my cubby-hole, though every time I began to think about lunch and peeped outside there seemed to be as many waiting as ever’.[7]
Impression of a GP Waiting Room: Mass Observation, Meet Yourself at the Doctors (1949)
Constant work and anxiety about the waiting room’s ‘vast unknown population’[8] left GPs feeling exhausted and stressed. ‘A life of uncertainty as regards the working events of a day’, one GP noted, ‘is nervously exhausting at all times’. Only with an appointments system was ‘the element of being in a hurry… eliminated’ and ‘a much calmer atmosphere’ established.[9]
Appointments thus enabled GPs to reduce daily physical and psychological strains, and offered greater control of time in their working and social life. They could now make time for dinners and professional development opportunities. Such pursuits also led enterprising practitioners to engage in the first out-of-hours companies and develop rotas for the burden of night calls.[10]
‘They are not just “the next patient, please”’
Such substantive change did not go unnoticed. Traditional GPs in particular expressed concerns about how appointments created psychological barriers to attendance for patients with uncertain symptoms, preventing the opportunity for early diagnosis.
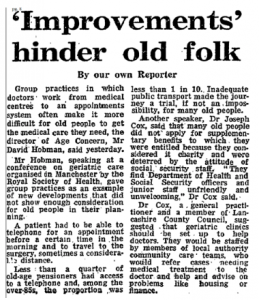
GPs also noted inequitable social consequences, pointing to poorer and elderly patients having difficulties making appointments. ‘The 3d for the telephone’, suggested one practitioner, was ‘an added expense to their budget’, whilst making timely journeys was made more challenging by reliance on public transport and greater geographical isolation.[11]
The Guardian, 12 December 1974, p. 8
Generally, however, patients seemed to accept new systems during the 1960s. Consumer bodies lobbied for them, and surveys revealed approval ratings as high as 98%. Primarily, patients appreciated reduced surgery waits (on average being halved) and liked being able to integrate appointments into their day, ‘shopping in what would previously have been waiting time in surgery’.[12]
Doctors also noted that patients appreciated having protected time with the GP. They even suggested that the work involved in securing a consultation meant had a ‘better understanding of the value of the time spent in consultation… emphasis[ing] the importance of the doctor’s advice’.[13]
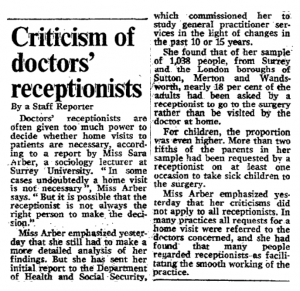
It was when appointments proved hard to come by that dissatisfaction manifested. In response, some patients lamented losing the traditional guarantee of same-day consultation, describing the queue as ‘much more humane’ than the delay and ministrations of ‘a dragon of a receptionist’.[14] Indeed, receptionists attracted considerable public ire.
Figure 1 The Times, 22 February 1978, p. 6
By contrast, some critics noted the changing experience of waiting, bemoaning declining ‘comraderie’ in the waiting room.[15] Whereas once waiting patients were collectively left out of sync with the rest of the social and economic community – to paraphrase Harold Schweizer – under appointments they were out of sync with one another.
*
By the time appointments systems nationally began to struggle, reverting to older temporal orders was almost inconceivable. Individual practices did abandon appointments after bad experiences, but generally too much financial, organisational and psychological investment had already been made.
The drive for choice and immediacy in appointments has undoubtedly pressurised GPs to be time conscious, and – as in the 1960s – has contributed to the undesirability of home visiting.
Though drawing lessons from the past is a dangerous activity, given the historical drift away from home visiting – and present pressures to access GPs on demand – it wouldn’t be a surprise to see home visiting hived off from GPs in the near future.
If it were, reintroducing home visiting to GPs after the act may well prove as difficult as removing the appointment. The other consequences of this change, though, are far more difficult to predict.
Notes
[1] S. Hadfield, ‘A field survey of general practice, 1951-2’, BMJ, 2:4838, (1953), p. 701. [2] N. Bosanquet and C. Salisbury, ‘The practice’ in I. Loudon, J. Horder and C. Webster, General Practice under the National Health Service, 1948-1997, (Oxford: Oxford University Press, 1998), p. 47. [3] ‘14 days to see your doctor’, The Lancet, 301:7809, (1973), 923. [4] E. Anthony, ‘The GP at the Crossroads’, BMJ, 1:4661, (1950), p. 1078. [5] J. Stevenson, ‘Appointment systems in general practice: do patients like them, and how do they affected work load?’, BMJ, 2:5512, (1966), p. 516. [6] Central Health Services Council Standing Medical Advisory Committee, The Field Work of the Family Doctor, (London: HMSO, 1963), p. 15. [7] R. Gordon, Doctor at Large, (London, Michael Joseph, 1955) [8] ‘Why are we waiting?’, Platform, (Basingstoke Consumer Group, October 1964), p. 28. [9] H. N. Levitt, ‘An appointment system in a single-handed general practice’, The Practitioner, 185 (1960), p. 213. [10] Bosanquet and Salisbury, ‘The practice’, pp. 58-9. [11] N. C. Horne, ‘An appointment system for use in general practice’, BMJ, (Supplement, 29 November 1952), p. 210. [12] D. Dean, I. M. Dean, B. R. Wilkinson, and R. McMurdo, ‘Appointment systems in general practice’, BMJ, 1:5434, (1965), 592. Also: J. M. Bevan and G. J. Draper, Appointment Systems in General Practice, (Oxford: Oxford University Press on behalf of the Nuffield Provincial Hospitals Trust, 1968), pp. 113-15 [13]The Field Work of the Family Doctor, p. 27.
[14] K. Johnstone, ‘Trying your patients’, The Guardian, 1 February 1979, 13. [15] J. Cunningham, ‘Doctors avoid ‘unnecessary’ calls’, The Guardian, 2 May 1973, 7.
Saturday, 30 November, 3:30 – 6:30pm, Women’s Art Library (WAL), Goldsmiths University Library
Join graphic novelists Sarah Lippett and Lucy Sullivan for an afternoon of discussion on the power of sequential narrative for approaching the topic of illness, loss and physical and mental health. Hosted in the context of the Women’s Art Library (WAL), curator and lecturer Samantha Lippett will chair a debate, paying specific reference to Sarah’s latest Jonathan Cape published graphic memoir, A Puff of Smoke, that explores her experience of growing up with an undiagnosed rare disease and Lucy’s graphic novel Barking, that draws upon her experiences of mental illness following the loss of her father in her early twenties. Framed within the genre of graphic medicine, together they will consider the radical potential of books like these to discuss the life topics that are often too complex for words alone. Followed by a Q&A.
There will also be a temporary display of the books and associated ephemera that will later be donated to the Women’s Art Library archives. Both graphic novels will be available to buy and free drinks for all.
With thanks to special collections librarian, Althea Greenan.
A Puff of Smoke (published by Jonathan Cape 7th November) is a graphic memoir about what it is like to grow up with an illness that no one can diagnose. Sarah Lippett spent eleven years suffering with symptoms from an unknown condition, until she was diagnosed with the rare disease Moyamoya at the age of 17.
For the month of November (1st – 29th November) an exhibition will be held at The Centre For Better Health that will explore the wider themes of the memoir.
Join Sarah as she talks through the process of revisiting her past and piecing it back together as a graphic memoir. The talk will be followed by a short workshop where participants are invited to create sequential narratives based on their own lived experiences. No drawing experience necesssary.
Read a recent Observer review of “A Puff of Smoke” book:
By continuing to use this website you consent to the use of cookies and your personal data as set out in our privacy policy. Close
Privacy & Cookies Policy
Privacy Overview
This website uses cookies to improve your experience while you navigate through the website. Out of these cookies, the cookies that are categorized as necessary are stored on your browser as they are as essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may have an effect on your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. This category only includes cookies that ensures basic functionalities and security features of the website. These cookies do not store any personal information.