Our PI Lisa is in conversation with ephemerajournal thinking through the temporal politics of COVID-19 and the ways in which pandemic conditions transform the affective dimensions of care work in Europe and US-America.
It is something of a foundational belief in the Sociology of Scientific Knowledge (and related fields) that knowledges are always shaped by the context within which they are constructed. Scientific knowledges are thus never independent of the social relations, economic structures, political pressures, ideological and tacit practices from which they emerged, and they are themselves cultural artefacts.[1]
Historians work with similar understandings about historical knowledge. Though articles or monographs do not routinely include historicisations of their own origins (though, note feminist histories like that by Catherine Hall and Carolyn Steedman), historians will usually recognise the circumstances of their text’s production in their acknowledgements.[2] Here they raise to the level of consciousness funding sources, intellectual interlocutors, social relationships and even some biographical detail to help make sense of where a particular work has developed.
The first page of acknowledgements by a certain author, who we shall call “M. Moore” to preserve their anonymity. That might be too obvious, let’s call them “Martin M.”
This is not to say that historians work unreflexively in relation to their origins, nor that they never publicly look to contextualise their own knowledge. Rather, they have tended to reflect most heavily on the relationship between past and present in historiographical and methodological texts.[3]
Recently the Waiting Times team has been thinking about how the current pandemic has been reshaping relationships to time (and care), which we will be sharing in a forthcoming dossier on COVID-19. It was in this context that I was reminded about E. H. Carr’s famous suggestion that history was an ‘unending dialogue between the present and the past’.[4] As historical and social subjects, in other words, historians are just as much a product of their particular time and place as those they write about, and our interpretations of the past will be inescapably influenced by our biographical, social and cultural relations.
Broadly speaking, historians have tended consider the relationship between the present of scholarship and the history produced in terms of large-scale social, economic and political formations and trends. How has a historian’s position in the social field shaped their view of the past? How might experiences of particular events or existence within specific cultural and political milieu shape the questions that are asked within research?
Regardless of how long the current measures of containment, delay and mitigation last, the impact of COVID-19 on psychosocial, economic and political life will likely be profound, and thus so will its effects on historical scholarship. Although it might be folly to think about precisely what these effects will be whilst we are still in the midst of the crisis – of a moment that might be an historical rupture and beginning of a new normal, or prove to be something far less monumental – it is nonetheless possible to consider how historical scholarship is already being reshaped. To explore how COVID-19 is already making history.
*
Perhaps the most overt ways in which the pandemic is influencing scholarship is in terms of disruption to intellectual networks and project temporalities.
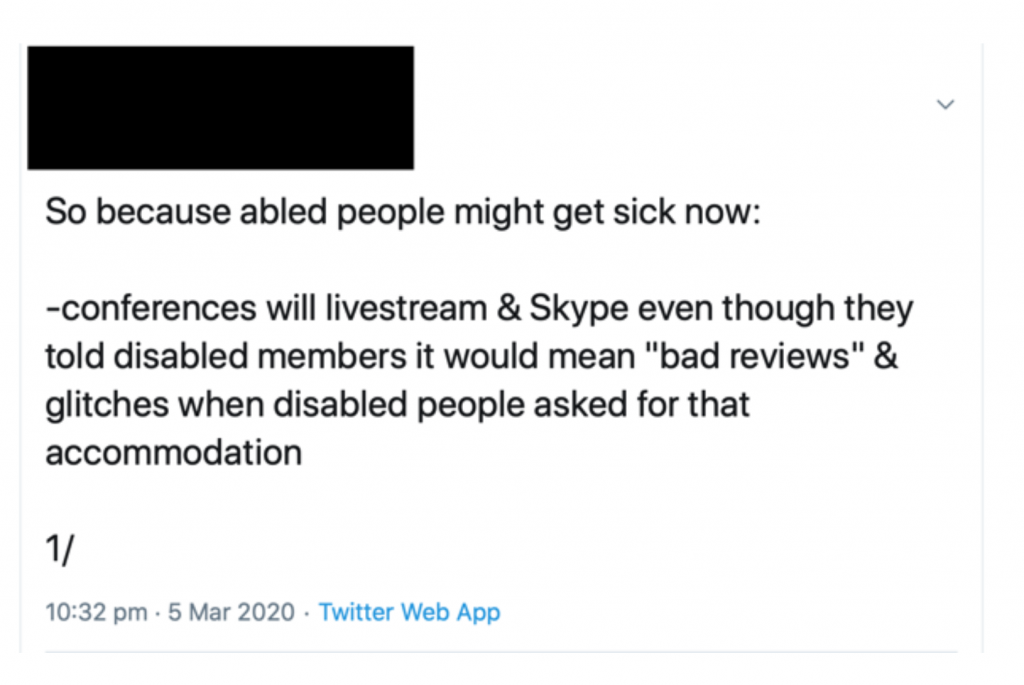
It might be tempting to point to the cancellation of conferences and reworking of seminars as a major consequence of COVID-19, and to consider how difficult it is to recreate opportunities for conversations and collaborations that tend to emerge from interaction outside of the formal conference room.
However, as disability activists and scholars with caring and familial responsibilities have pointed out, these issues are long-standing. It should be a matter of shame that it has taken a global pandemic to force able-bodied academics to think seriously about alternative ways of working, when this has been so long denied to colleagues unable to be physically present at large, and often distant, events.
Instead, a problem more directly caused by the pandemic is how COVID-19 has radically disrupted postgraduate and PhD research, and will potentially reduce the time available to undertake ongoing projects. At the time of writing, some funding bodies have so far shown a willingness to ensure no cost extensions in proportion to the disruption experienced, but considerable anxiety and uncertainty still exists, and the internal research leave and fixed contract arrangements of individual universities are being addressed idiosyncratically. The absence of a sector-wide response – of guaranteed secure employment at (or above) present levels of pay for casualised staff – has begun to generate political action under the banner of a Corona Contract. However, even if agreed, the personal circumstances of researchers change over time, and their capacity to undertake the same work may well be altered in the future. The knowledge produced will thus likely be substantively different as a result.
Similar analyses can be applied at the level of teaching. As was made clear at the Modern British Studies conference last August, history modules are already being shaped by the short fixed-term, zero-hour contracts spreading throughout academia. This has often reduced preparation time and opportunities for scholars to create their own offerings, leading to modules being inherited and reworked where possible by temporary staff. Individual universities have used COVID-19 as legitimation for laying off staff or refusing to continue contracts of fixed-term employees, and together with social distancing the landscape of teaching looks very different as a result.
*
Of course, the pandemic is also shaping the knowledge it is possible to produce at the level of sources and methods.
Closures of archives and libraries has ensured a majority of resources remain inaccessible, and de facto quarantine is altering the way we can undertake oral historical work. (Given that the direction of an encounter is often shaped by the embodied interaction of interviewer and interviewee constructing the interview together in the same room, it is likely that even online interviewing will produce different testimonies.)
Some textual and visual materials are available online, partly due to digitisation and partly due to the increasing use of the internet as historical object and source.
For instance, texts that are available digitally and made keyword searchable can grow in epistemological importance. Equally, engagement with uncatalogued materials becomes impossible, and the assessment of a source’s materiality – its physical substance, potential sensory responses, clues to its production – are also precluded or made more difficult. In this sense the pandemic risks compounding historians’ existing reliance on the narrow range of sources that have managed to survive, and which have often been produced by social elites and from positions of (often violent) power. We will require further innovation in approaches and methodologies to avoid reproducing historical violence in the present.
At the same time, public and political discourses of healthcare, disease and contagion – as well as experiences of illness and practices of social distancing and self-isolation – are also altering how we might read and interpret our sources.
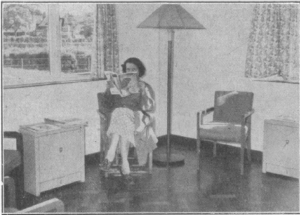
At a very basic level, I am currently revisiting my own work on waiting rooms. Under present conditions, materials relating to concern of infection are beginning to stand out more. References to feeling disturbed or diminished by waiting with patients with ‘hacking coughs’, for example, take on greater resonance, as do recollections of the way such anxieties shaped practices of attending surgery and sharing the time of waiting.
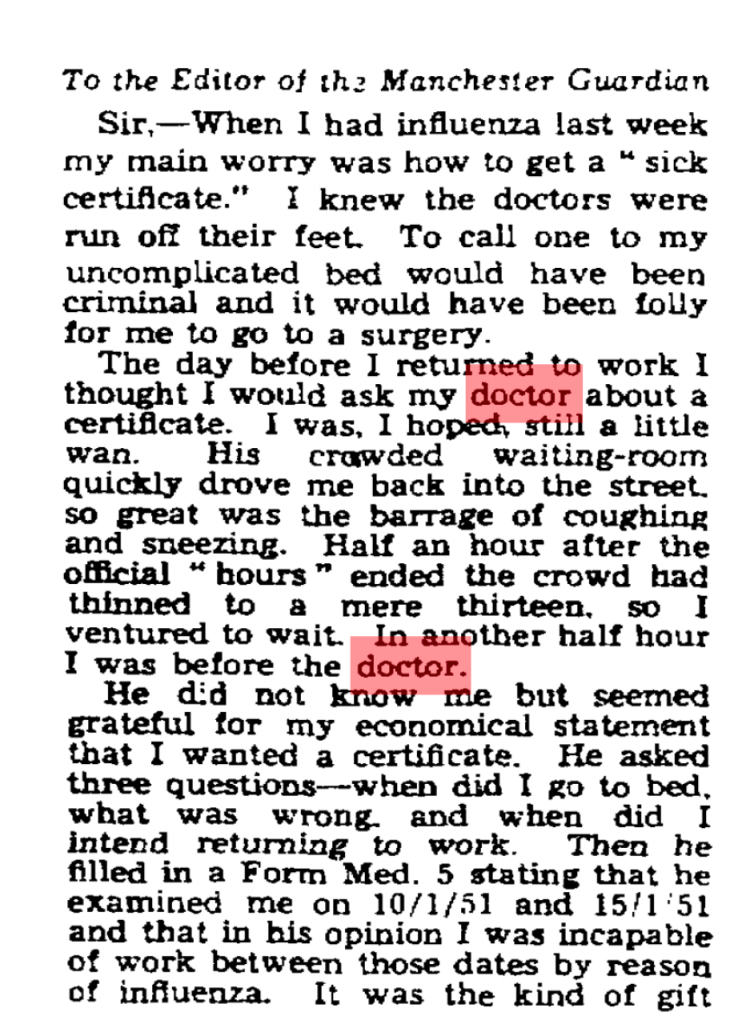
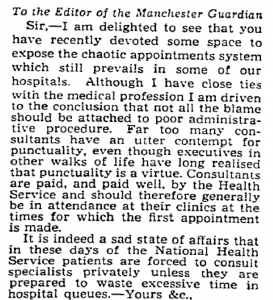
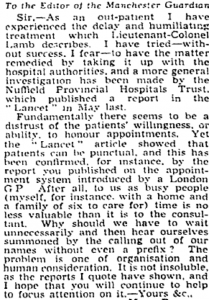
Take, for instance, one letter to the Manchester Guardian in 1951 about trying to collect a sickness certificate:
‘Ministries and medicine’, Manchester Guardian, 17 January 1951, p. 4
The day before I returned to work I thought I would ask my doctor about a certificate. I was, I hoped, still a little wan. His crowded waiting-room quickly drove me back into the street, so great was the barrage of coughing and sneezing. Half an hour after the official “hours” ended the crowd had thinned to a mere thirteen, so I ventured to wait. In another half an hour I was before the doctor.
Previously, I may have read this in terms of anxieties of waiting for – and consulting – the doctor when appearing healthy, in relation to the performativity of sickness. Equally, the source raises questions about the length of acceptable waiting, the responsibilities that doctors had to attend their patients after surgery hours, and the role of the medical profession in sick note certification. Even though I would have registered the disquiet with the waiting room as a source of infection, the fear of contagion would not have hit home in the same way.
Similar alterations in my interpretation have manifested in relation to GP’s frustrations with patients bringing in “dirt” to their waiting rooms. I have previously read such complaints in highly symbolic terms, in line with my interest in how discourses of dirt and cleanliness have been historically racialised and classed. Now, however, I am paying greater attention to dirt’s materiality. Though GPs’ irritations cannot be conceptually divorced from “dirt’s” cultural values, my own anxieties around the ongoing pandemic has made me appreciate the medical concern with hygiene embedded in GP’s choices of easy-to-clean materials for redecorating waiting in a period of regular infectious disease outbreaks.
Finally, even should the present proscriptions around “staying home” be eased, and libraries and archives swiftly reopen, the emotional experience of being in and using such spaces will also have been altered.
I already feel much more “exposed” simply going to a small supermarket, so I can only imagine that the experience of using public transport, sharing the space and time of research with others, and interacting with well-handled resources will be radically different for some time. To presume that such affective responses will not alter how I interact with historical sources (the time I can bear to be with them, how much more I rely on digitised versions) or the sorts of questions I will ask of them would be disingenuous.
Of course, even as I write many people literally cannot afford to avoid public transport or working away from home
*
There are, of course, much more complicated ways to think historically about epidemics, time and care in relation to scholars’ experiences of the present moment, and undoubtedly our teaching on history of disease and medicine modules will also be shaped by our students’ personal perspectives on their lockdown and social distancing.
Moreover, that I – and scholars like me – are only beginning to consider such questions seriously can itself be historicised.
This very reflection is the product of my having grown up in a period and place in which my privilege as a heterosexual, white (once working-, now solidly middle class) male living in Britain has afforded me protection – not simply from the epidemics that have tended to exist geographically and socially “elsewhere” (from HIV/AIDs to Ebola) but also from the structural violence that has consistently distributed disease disproportionately among the poorest and those most discriminated against in Britain (and globally). Even now, my positionality is proving protective, as underlined by reports that BAME communities are suffering disproportionate mortality from COVID-19.
Given the racial, class and gender disparities among the historical profession, I suspect that my experiences may be widely shared.
Nonetheless, whether explicitly discussed in acknowledgements, expressed within the subjects, questions and contours of research, reflected in how we organise and practice intellectual network formation, or manifest in the conditions within which teaching is delivered, the effects of COVID-19 on the present and future of historical scholarship will likely be widespread and significant. As such, though academic departments are by no means the only source of historical knowledge and narrative, it is fair to say that the present pandemic is also rewriting the past.
Notes
[1] For classics in the field and useful reviews: S. Shapin and S. Schaffer, Leviathan and the Air Pump: Hobbes, Boyle and the Experimental Life, (Princeton: Princeton University Press, 1985); S. Woolgar and B. Latour, Laboratory Life: The Construction of Scientific Facts, (Princeton: Princeton University Press, 1986); K. Knorr Cetina, Epistemic Cultures: How the Sciences Make Knowledge, (Cambridge, Mass: Harvard University Press, 1999); L. Daston and P. Galison, Objectivity, (New York: Zone Books, 2010).
[2] The most self-conscious example I have seen is the preface to a history on international development and the social sciences, which begins: ‘this book as much as the institutions which are its subject, comes out of a particular history, a certain intellectual climate, and specific funding possibilities’: R. M. Packard and F. Cooper (eds), International Development and the Social Sciences: Essays on the History and Politics of Knowledge, (Berkeley: University of California Press, 1997), p. vii. For examples of texts firmly grounded in the historian’s own positionality: C. Hall, White, Male and Middle Class: Explorations in Feminism and History, Cambridge: Polity Press, 2007 [1992]); C. Steedman, Landscape for a Good Woman: A Story of Two Lives, (London: Virago, 1986).
[3] For instance: A. Green and K. Troup, The Houses of History: A Critical Reader in History and Theory, Second Edition (Manchester: Manchester University Press, 2016); L. Jordanova, History in Practice, Third Edition, (London: Bloomsbury Academic, 2019).
[4] E. H. Carr, What is History?, Second Edition (London: Penguin, 1990 [1961]), p. 30.
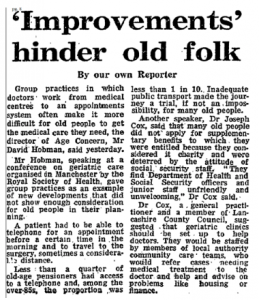
‘My own doctor is a charming man when one can eventually win an appointment to see him’: accessing the GP and the time of care in British general practice
Although, according to recent NHS data, on average only 1% of total primary care appointments were for home visits, the motion provoked a considerable backlash among patient groups, senior healthcare professionals, the press and Government ministers.
Critics broadly focused on the capacity for severely ill and immobile patients to access the GP, whereas supporters argued that GPs ‘no longer have the capacity to offer’ visits. At its heart, in other words, were questions about for whom and for what GPs should reasonably make time.
As my recent work on appointments systems is revealing, GPs’ time and patients’ rights of access to care have formed a central object in public debate since the foundation of the NHS. By contrast to the current proposals, however, the emergence of full-time appointments systems for surgery sessions in general practice generated far less initial resistance, despite affecting a far greater proportion of the practice population.
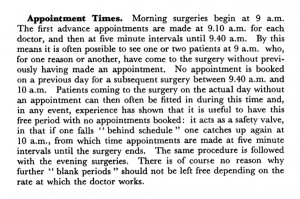
‘Much of the overwork of which doctors complain is due to lack of proper business methods’
The first decades of the NHS witnessed a considerable change in how people waited for a GP consultation.
In the early 1950s, only 2% of British general practices employed full time appointments systems for their surgery sessions.[1] In the vast majority of practices, those patients wishing to see the doctor could simply arrive at the premises during surgery hours and wait to be seen in turn. Even practices with appointments systems quietly reserved part of the surgery session for patients arriving without an appointment.
From A. E. De La T. Mallett, ‘An appointment system in a group practice’, College of General Practitioners Research Newsletter, 3:8 (1955), 113-18
Finally, for those too ill to come to the surgery, visits were common; around a quarter of consultations on average occurred in patients’ homes.[2]
By the early 1970s this situation had dramatically altered. Around 80% of practices now employed full-time appointments systems.[3] Crucially, changes to NHS rules empowered doctors to defer treating patients who they felt were not in need of immediate attention. Patients were thus increasingly unable to access the doctor on demand without an appointment. A wait for the doctor might stretch to several days if one was unavailable immediately.
As with contemporary discussion around home visits, GPs’ concern with time pressure generated interest in appointments systems. Following the creation of the NHS, many GPs bemoaned having ‘much more work’ and feeling like they were ‘chasing [their] practice downhill all the time with no hope at present of ever catching up’.[4] As a result, many doctors sought organisational innovation to achieve ‘more economic use of … time and energy’.[5]
Notably, one particular attraction of new systems was that they might ‘reduce the demand for visits’, as reduced crowding and waiting times could make surgery attendance less taxing.[6] The time saved by reduced travelling could be put to use elsewhere.
Efficiency was not the sole factor motivating GPs to take up appointments systems, however. Traditional arrangements, for instance, could lead to late-running surgeries – any patient who arrived before doors closed had a right to be seen. As one satirical novel put it: ‘the patients came steadily to my cubby-hole, though every time I began to think about lunch and peeped outside there seemed to be as many waiting as ever’.[7]
Impression of a GP Waiting Room: Mass Observation, Meet Yourself at the Doctors (1949)
Constant work and anxiety about the waiting room’s ‘vast unknown population’[8] left GPs feeling exhausted and stressed. ‘A life of uncertainty as regards the working events of a day’, one GP noted, ‘is nervously exhausting at all times’. Only with an appointments system was ‘the element of being in a hurry… eliminated’ and ‘a much calmer atmosphere’ established.[9]
Appointments thus enabled GPs to reduce daily physical and psychological strains, and offered greater control of time in their working and social life. They could now make time for dinners and professional development opportunities. Such pursuits also led enterprising practitioners to engage in the first out-of-hours companies and develop rotas for the burden of night calls.[10]
‘They are not just “the next patient, please”’
Such substantive change did not go unnoticed. Traditional GPs in particular expressed concerns about how appointments created psychological barriers to attendance for patients with uncertain symptoms, preventing the opportunity for early diagnosis.
GPs also noted inequitable social consequences, pointing to poorer and elderly patients having difficulties making appointments. ‘The 3d for the telephone’, suggested one practitioner, was ‘an added expense to their budget’, whilst making timely journeys was made more challenging by reliance on public transport and greater geographical isolation.[11]
The Guardian, 12 December 1974, p. 8
Generally, however, patients seemed to accept new systems during the 1960s. Consumer bodies lobbied for them, and surveys revealed approval ratings as high as 98%. Primarily, patients appreciated reduced surgery waits (on average being halved) and liked being able to integrate appointments into their day, ‘shopping in what would previously have been waiting time in surgery’.[12]
Doctors also noted that patients appreciated having protected time with the GP. They even suggested that the work involved in securing a consultation meant had a ‘better understanding of the value of the time spent in consultation… emphasis[ing] the importance of the doctor’s advice’.[13]
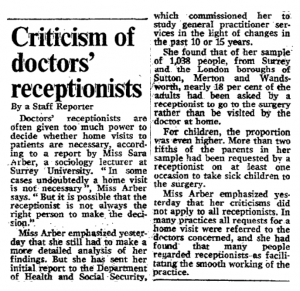
It was when appointments proved hard to come by that dissatisfaction manifested. In response, some patients lamented losing the traditional guarantee of same-day consultation, describing the queue as ‘much more humane’ than the delay and ministrations of ‘a dragon of a receptionist’.[14] Indeed, receptionists attracted considerable public ire.
Figure 1 The Times, 22 February 1978, p. 6
By contrast, some critics noted the changing experience of waiting, bemoaning declining ‘comraderie’ in the waiting room.[15] Whereas once waiting patients were collectively left out of sync with the rest of the social and economic community – to paraphrase Harold Schweizer – under appointments they were out of sync with one another.
*
By the time appointments systems nationally began to struggle, reverting to older temporal orders was almost inconceivable. Individual practices did abandon appointments after bad experiences, but generally too much financial, organisational and psychological investment had already been made.
The drive for choice and immediacy in appointments has undoubtedly pressurised GPs to be time conscious, and – as in the 1960s – has contributed to the undesirability of home visiting.
Though drawing lessons from the past is a dangerous activity, given the historical drift away from home visiting – and present pressures to access GPs on demand – it wouldn’t be a surprise to see home visiting hived off from GPs in the near future.
If it were, reintroducing home visiting to GPs after the act may well prove as difficult as removing the appointment. The other consequences of this change, though, are far more difficult to predict.
Notes
[1] S. Hadfield, ‘A field survey of general practice, 1951-2’, BMJ, 2:4838, (1953), p. 701. [2] N. Bosanquet and C. Salisbury, ‘The practice’ in I. Loudon, J. Horder and C. Webster, General Practice under the National Health Service, 1948-1997, (Oxford: Oxford University Press, 1998), p. 47. [3] ‘14 days to see your doctor’, The Lancet, 301:7809, (1973), 923. [4] E. Anthony, ‘The GP at the Crossroads’, BMJ, 1:4661, (1950), p. 1078. [5] J. Stevenson, ‘Appointment systems in general practice: do patients like them, and how do they affected work load?’, BMJ, 2:5512, (1966), p. 516. [6] Central Health Services Council Standing Medical Advisory Committee, The Field Work of the Family Doctor, (London: HMSO, 1963), p. 15. [7] R. Gordon, Doctor at Large, (London, Michael Joseph, 1955) [8] ‘Why are we waiting?’, Platform, (Basingstoke Consumer Group, October 1964), p. 28. [9] H. N. Levitt, ‘An appointment system in a single-handed general practice’, The Practitioner, 185 (1960), p. 213. [10] Bosanquet and Salisbury, ‘The practice’, pp. 58-9. [11] N. C. Horne, ‘An appointment system for use in general practice’, BMJ, (Supplement, 29 November 1952), p. 210. [12] D. Dean, I. M. Dean, B. R. Wilkinson, and R. McMurdo, ‘Appointment systems in general practice’, BMJ, 1:5434, (1965), 592. Also: J. M. Bevan and G. J. Draper, Appointment Systems in General Practice, (Oxford: Oxford University Press on behalf of the Nuffield Provincial Hospitals Trust, 1968), pp. 113-15 [13]The Field Work of the Family Doctor, p. 27.
[14] K. Johnstone, ‘Trying your patients’, The Guardian, 1 February 1979, 13. [15] J. Cunningham, ‘Doctors avoid ‘unnecessary’ calls’, The Guardian, 2 May 1973, 7.
Providing effective treatment and support for mental distress is a stated government aim. Within low-income communities, use of antidepressant medications is relatively high, but current strategies frame mental distress as an individual psychological problem, masking the factors that are often the root causes of suffering e.g. social isolation, unemployment.
The lead author of the report is Dr Felicity Thomas, Senior Research Fellow on the Cultural Contexts of Health, and a Senior Research Fellow in the Medical School at the University of Exeter.
Whether in pop culture or academic work, time and space have often been inextricably linked. Though the Waiting Times team has been thinking about temporality in ways that breaks – or at least complicates – this connection, one space that I have been thinking about recently has been the general practice waiting room.
The waiting room as an historical space
As work by the Cultural Histories of the NHS project suggests, contemporary experiences and associations of NHS waiting are often shaped by its material elements, not least the chairs and signs that populate its waiting rooms.
The work I have been doing has been to consider how such spaces and associations came to be. Much like the medical appointment, the waiting room is an historical construction. It is a space which only began to receive sustained public attention in Britain with the collectivisation of healthcare funding under National Health Insurancein 1913, and which practitioners only began to think about substantively following the creation of the health service after 1948.
The creation of the NHS was particularly important, with the removal of insurance principles or payment barriers increasing the demand on premises that had not been designed to hold large numbers of patients: many practices in 1948 were in small converted shop premises or in a GP’s house. The latter might have the dining room as a waiting area, but patients waiting outside either type of premises was not uncommon.
The NHS also made criticisms of health services a problem for central government – leading politicians to apply pressure for reform – as well as drawing much firmer lines between general practice and hospital practice, forcing GPs to think about how to distinguish themselves professionally.
The post-war settlement and the waiting room
The way that the NHS brought attention to the waiting room often meant that discussions were framed in relation to the promises of – and discontents with – what some historians refer to as the post-war settlement.
With regards to healthcare, elite practitioners and organised professional bodies like the British Medical Association had opposed the NHS as conceived by the Labour government in 1948. Among other things, they feared that state employment would result in a loss of income, professional freedom, and unmediated professional-patient relationships.
GPs in particular continued to criticise the new service into the early 1950s.
Some complained about a loss of class deference and professional status, of being treated by patients as servants or ‘suppliers of medicines’ rather than as a medical advisers or even as friends.
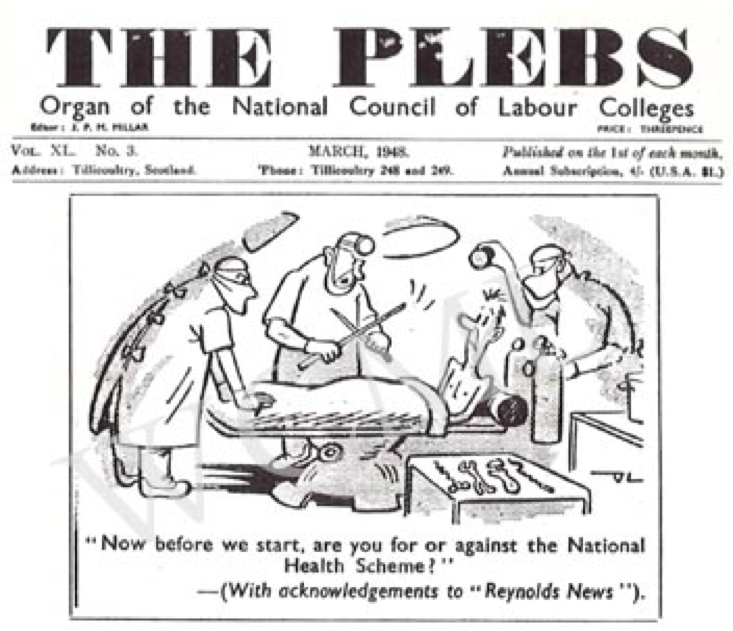
They also argued that, by removing financial barriers to care, the NHS created demanding and entitled patients. Patients would allegedly enter the consulting room ‘‘to tell us what is wrong and what [they] want for it’.
Manchester Guardian, 18 October 1949.
These anxieties about status and the shifting relations of medicine were played out in discussions of waiting rooms.
Reports were sent to central government departments about patients who would ‘tear out pages of periodicals in the waiting room, grind sticky sweets into the carpet, take cushions, and even carve their initials on the furniture’. One GP appealed to the Ministry of Health to make ‘it quite clear to the general public that a doctor’s waiting-room is not a place of public entertainment, but rather a place where people are expected to behave with a certain amount of respect and decorum’.
The focus on patient behaviour and deference was indicative of the class-bound anxieties of some GPs, many of whom would have previously had separate entrances and waiting spaces for private patients and those receiving publicly-funded care. No longer able to segregate their patients, some doctors were still so concerned about working class patients bringing dirt into waiting rooms that they even used interior design to prevent ‘greasy heads’ marking walls, and praised the durability of flooring to stand up to workmen’s boots.
The domestic and middle-class ideals of GP waiting rooms Supplement to the British Medical Journal, 6 November 1954
The challenges of writing histories of the waiting room
There is still much to explore about how waiting rooms were thought about and redeveloped over the twentieth century. However, researching the subject so far has not proven straightforward.
Methodologically, I have faced problems familiar to many social and cultural historians. The “archives” of general practice waiting rooms are hardly substantial, and have been largely created or curated by medical professionals, civil servants, and media editors. Equally, their materials are predominantly composed of digressions about waiting rooms made in discussions about other topics, or are made up of complaints that reveal expectations and social norms only by their absence or negation.
The dominance of complaints from “establishment” groups, however, has also posed other challenges, causing me to reflect on my own subjectivity and affective responses to sources.
As a social historian, I share my field’s political and intellectual sympathies to histories of marginalised groups, as well as its critical disposition to power and professional self-interest. Likewise, as someone who has grown up with – and been a long-term beneficiary of – the NHS, I have been interpellated by its core ideals (if not lived practice) of universal healthcare, free at the point of use.
As a result, GPs’ grievances initially struck me as exaggerated, underpinned by a sense of superiority to patients, and indicative of an opposition to any form of egalitarianism from professionals with considerable class privilege.
Indeed, surveys conducted at the time provided some support for this reading, with one prominent medical observer noting that ‘some general practitioners are so easily irritated by such an attitude [of entitlement and lack of respect among patients] that they are apt to think it more widespread than it actually is’.
My first engagement with these materials, therefore, was to read criticisms primarily for the way they provided insight to the reception of the post-war welfare state, and for the strategic purpose the played inprofessional and political projects.
Nonetheless, further exploration and consideration has brought home the importance of maintaining critical reflection on my own subjectivity and affective responses.
Historically, it was not just doctors who were sceptical or anxious about the NHS. State provision had not been welcomed by everyone.[1] For instance, though many were quickly convinced of the NHS’s advantages, a significant proportion of the British public were initially concerned about the potential loss of ‘the personal touch’ in state-funded medicine.
Moreover, though there is a clear element of performativity in GPs’ complaints, in reading them differently I have also begun to tease out insights into the culture of the early health service – the way its proposed radicalism was filtered through inherited buildings and beliefs, the presumptive middle-class norms behind ideas of universality, and the ways that attitudes towards patients were slowly built into the very fabric of the service.
Even more varied readings are possible, ones that might reveal more about the everyday life of post-war Britain. Complaints about demanding patients, for example, could provide insight into the complexities of the psychological life of traditional middle-class groups in a period of rising affluence but concern about relative decline. Similarly, reading discussions about nailed boots and greasy heads for indicators of patient behaviour might generate insight into the changing nature of work and housing, or shifting social norms about self-presentation in public spaces, if read over time.
However, changing the way I engage with sources and the questions I ask has required more than a change in methodology or conceptualisation.
I have had to maintain an awareness of my own position in academic and political fields. I have had to reflect on how my work has been informed by my own psychological investments in the NHS and its proposed values, as well as by my attachment or critical disposition towards certain professional groups.
Of course, undertaking practices of self-reflection is not the same as striving for “objectivity”, or somehow overcoming my position as an historically-formed subject. Instead, it is to realise that a critical disposition towards the historian’s subjectivity can open up new questions and new avenues for research.
Who would have thought that even just thinking about waiting rooms (rather than being forced to wait within one) could encourage such existential questions? (Bergson, put your hand down – no-one likes a show-off.)
Henri Bergson – Philosopher, Smart-Ass, Terrible Queuing Partner
Dr Martin Moore is the historian on the Waiting Times project.
The aim was to use the intense interest in the service generated by the 70thanniversary to bring historical reflection on present day concerns.
The day encouraged discussion among the diverse participants, with exchange structured by three academic papers and provocations. The first, by Jonathan Barry (University of Exeter), provided insight into how the major broadsheet press treated the creation of the health service, whilst the second by Andrew Seaton (New York University), reflected on the everyday experiences of life on the wards of NHS hospitals. Among other things, these papers raised important points about the way that support from the press and middle-class users in particular was essential to securing the political future of the nascent service.
My own paper looked at the different ways that the politics of welfare and values attached to the NHS influenced patient perceptions of waiting for referrals and appointments in surgery and outpatient departments.
Of course, frustrations with waiting were often underpinned by agonising uncertainty, physical pain, and a more general anxiety about wasting time that might have been better used elsewhere.
Nonetheless, the promises of – and discontents with – the values of the welfare state and universal health care structured interpretations of waiting. For instance, for some of the newly enfranchised, queuing for spectacles was seen as the result of the egalitarian return of the repressed. By contrast, for others, waiting in outpatients for hours was seen as a failure to fulfil promises to “universalise the best”, and forced people into the arms of private medicine.
Manchester Guardian, 13 January 1953
The promise of speed in alternatives to the NHS (which is itself built on the exclusion of large-scale demand) is still an ever present in marketing campaigns for providers.
BUPA Website, c. September 2018
One issue I wanted to give particular emphasis in my discussion, however, was how the early NHS had failed to incorporate patient perspectives within its structures. The NHS was essentially created as a way to bring doctors and healthcare staff into state services and thus expand access to a comprehensive and equitable health service to all.
Official government pamphlet promoting launch of the NHS, c. 1948
Yet, although grounded in socialist and social democratic traditions (among other influences), the creators of the service paid little attention to democratic input other than through the selection of governments over election cycles.
Patients and their families rarely had direct input into the design of services in the early years of the NHS, and there were no formal mechanisms for raising complaints or providing patient perspectives until after scandals in long stay hospitals in the late 1960s and early 1970s.
Prior to then, if patients were lucky complaints about waiting might be considered institutionally, but the few internal investigations I have seen all found “no case to answer”. In such circumstances, we can see patients’ letters to the press as arising out of frustrations having no alternative route for expression.
I wanted to outline this history at the event to raise questions around accountability and inclusion that exist outside the usual managerial frames of audits and surveys. I also wanted to ask participants on the day about how we might build the local components of the NHS as democratic institutions, incorporating patient expectations into services in a way that might escape the traps of “rights and responsibilities” discourses.
Asking these questions, I believe, might have some import for our contemporary understanding of waiting. If, as my paper suggested, our experience of waiting is intertwined, at least in part, with historically-specific ideas of what is owed, then perhaps our waiting might take on a different set of meanings if those who are waiting are a part of the promise-making process.
These themes, along with many others raised by the workshop participants, will form part of an ongoing discussion that we hope to have over the coming few years.
Dr Martin Moore is the historian working on the Waiting Times project.
Whilst “wasting time”/“productively searching for historic pop culture representations of waiting” this week [delete as appropriate], I happened upon an episode of the sketch show, A Bit of Fry and Laurie from the early 1990s. In one of their “talking head” parodies, Hugh Laurie’s character comments:
“Well, we had our first child on the NHS. And had to wait nine months…
…Can you believe it?”
At the risk of proving E. B. White correct (and ‘killing the frog’), on the surface the joke played upon well-known durations of pregnancy, and invites us to laugh at the commentator’s ignorance.[i] The skit, however, also lampooned a certain type of caricatured middle class NHS user: one who approached health care with consumerist expectations, and who was prone to making (in this case, unreasonable) complaints about public service inefficiency.
The sketch, in other words, was a response to changing popular and parliamentary approaches to health care.[ii] As Sally Sheard and Alex Mold (respectively) have demonstrated, political and managerial attention to health service waiting undoubtedly intensified during the 1980s and early 1990s, and the period witnessed an individualisation of patient consumerism more generally.[iii]
Yet, as early Waiting Times research is showing (and as suggested by the ageing Laurie’s character), patient dissatisfaction with delays and waiting had been a feature of the NHS since its beginning.
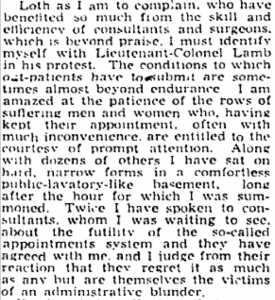
During the late 1940s and early 1950s, for instance, Britain’s newspapers carried numerous letters from patients discussing their experiences of waiting for consultations in general practice and hospital outpatients, as well as deploring the waiting lists for hospital appointments, admission, and treatments.
Patients attending for consultations described waiting as ‘irksome’, ‘inconvenien[t], and ‘endless’.
Most did not explain why they were displeased at this wasted, interminable time, perhaps assuming the reasons to be obvious. However, we can find glimpses.
Some correspondents hinted that frustration arose from misaligned public and private schedules. They had multiple personal and social responsibilities, and time became an economic resource: time spent waiting was time taken away from other tasks.[iv]
There were, however, more symbolic concerns. The prioritisation of medical time over the patient’s own was a source of irritation, especially when subsequent encounters were depersonalised.
‘Outpatients at hospital’, Manchester Guardian, 3rd January 1953
Complainants often criticised the self-interestedness of doctors for appointment system failures and expressed dismay at clinicians for arriving late.
Yet, even when the doctors were considered courteous and blameless (with administrators were positioned as the villains of the piece), correspondents suggested that the squalor of public environments of waiting compounded their physical and psychological distress, and made their experiences almost unbearable.
‘Outpatients at hospital’, Manchester Guardian, 3rd January 1953
Of course, early patient responses to waiting also varied.
As with newspapers and political parties, some letters linked their quotidian experiences to broader political points.[v]Letter writers and Mass Observation respondents both echoed public narratives that queues were either the inevitable result of iniquitous, incompetent socialism, or temporary, and signs of egalitarian health care extending to persons previously priced-out of access. Others were tentatively resigned to waiting simply being a part of mass medical practice.
Yet, whether incensed or accepting (or simply mildly irritated), the vast majority of correspondents to publications and surveillance machinery, offered possible solutions.
Commentators suggested disaggregating appointments (rather than block booking everyone for the start of the clinic) and providing better information on the order of patients to be seen, as well as suggesting that waiting patients ‘equip themselves with a book or piece of knitting’ (‘it seems only common prudence’).[vi]
Like the Doctor looking for a fez, one correspondent seemingly got a little carried away in their endeavour, suggesting: ‘the waiting period should be made more pleasant by decorating the walls more attractively, better use of light, plenty of up-to-date magazines, books etc., flowers and pot plants, even an aquarium or small aviary, but most of all an air of cheerfulness and efficiency about the place.’[vii]
Although likely containing only the viewpoints of a very specific subset of the general population, these letters and survey responses thus offer considerable insight into waiting in the early NHS.
They shed light into the power dynamics at play in British medicine (for instance, whose time was prioritised). They highlight how modernist drives to “synchronise” individual, public, and institutional time had ordered the lives of mid-century patients and practitioners, but caused psychological distress when disturbed.[viii]
They also offer a glimpse into the longer history of quotidian experiences of waiting as slow and endless, and demonstrate the importance of comportment and environment to such perceptions.
Crucially for our appreciation of ‘80s and ‘90s sketch shows available on popular streaming services, however, they also underscore how political opposition to public services, and complaints about waiting in them, are as old as the services themselves.
Dr Martin Moore is the historian working on the Waiting Times project.
Notes
[i]White reportedly said: “humor can be dissected, as a frog can, but the thing dies in the process and the innards are discouraging to any but the pure scientific mind”. Those innards would likely be purchased by high-end restaurants and served on a bed of puréed dreams, now, however…
[ii]The show itself was well-known for lampooning older traditions of conservative morality, as well as what were then termed “Thatcherite” views of business and national services. It once suggested that Mrs Thatcher herself could be easily replaced by a coat hanger (to the nation’s benefit), and satirically created its own “Comedy Charter”, ‘a basket of top proposals’ to enable the viewer to complain and thus maintain the show’s quality and standards. The latter was a conscious play on the spate of such documents that followed John Major’s “Citizen’s Charter”, one of which was a “Patient’s Charter” that included minimum waiting times for patients.
[iii]S. Sheard, ‘Space, place and (waiting) time: reflections on health policy and politics’, Health Economics, Policy, and Law, (Early Access Online); A. Mold Making the Patient Consumer: Patient Organisations and Health Consumerism in Britain, (Manchester: Manchester University Press, 2015).
[iv]G. Horobin and J. McIntosh, ‘Time, risk and routine in general practice’, Sociology of Health and Illness, 5:3, (1983), 312-31.
[v]J. Moran, ‘Queuing up in Post-War Britain’, Twentieth Century British History, 16:3, (2005), 283-305.
[vi]B. M. Fleming, ‘Hospital out-patients’, Manchester Guardian, 13thJanuary1953, p. 2.
[vii]H. Sumerfield, ‘Out-patients at hospital’, Manchester Guardian, 8thJanuary1953, p. 4.
[viii]B. Adam, Timewatch: The Social Analysis of Time, (Cambridge: Polity Press, 1995); Jacques Le Goff [translated by Arthur Goldhammer], Time, Work and Culture in the Middle Ages, (Chicago: University of Chicago Press, 1980).
By continuing to use this website you consent to the use of cookies and your personal data as set out in our privacy policy. Close
Privacy & Cookies Policy
Privacy Overview
This website uses cookies to improve your experience while you navigate through the website. Out of these cookies, the cookies that are categorized as necessary are stored on your browser as they are as essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may have an effect on your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. This category only includes cookies that ensures basic functionalities and security features of the website. These cookies do not store any personal information.